Shoulder Injury Related to Vaccination (SIRVA)
Conclusion | Evidence | Proposed Biological Mechanism | Prevention | References
Conclusion
Vaccines can cause SIRVA (shoulder injury related to vaccination) when administered incorrectly.
Evidence
The primary evidence supporting a causal association includes clinical assessment and imaging studies of the area where the injection occurred. Injection in the upper third of the deltoid can result in inflammation of the subacromial(deltoid) bursa, the supraspinatus muscle, tendons, or bony structures [1,2,3]. Damage to the radial nerve can occur when the injection is given too low [4]. In 2012 the Institute of Medicine (IOM) determined that clinical evidence was sufficient to determine that vaccine injection was a contributing cause of deltoid bursitis [5].
Proposed Biological Mechanism
SIRVA has occurred following several different vaccines, and is caused by an immune-mediated inflammatory response [1-3,5,6]. The most common contributing factors include administration in the upper one-third of the deltoid muscle and injection deep enough to pass through the muscle to the underlying tissues. SIRVA has become the most common injury awarded compensation by the Vaccine Injury Compensation Program (VICP)[6]. Approximately 80% of individuals who develop SIRVA are female, and low body mass index is a risk factor because of smaller muscle mass [6].
Prevention
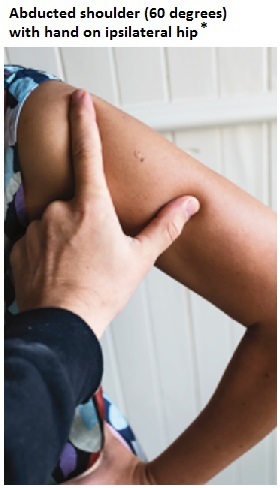
SIRVA can be prevented by administration of intramuscular vaccines into the MIDDLE of the deltoid muscle at a 90° angle using an appropriate length needle [CDC]. The best method for identifying the middle of the deltoid muscle was developed by Cook in Australia and involves the following steps [7,8].
1. Have the patient put their hand on their hip with the shoulder extended about 60 degrees.2. Put your index finger on the acromion and thumb at the deltoid insertion at the middle of the humerus.
3. Administer the vaccine in the middle of the triangle (see figure) using an appropriate needle length for the patient [9,10].
For many years training institutions incorrectly indicated that measuring 2 to 3 fingerbreadths below the acromion process would identify the middle of the deltoid muscle. Unfortunately, using the fingerbreadth method results in the administration of vaccines in the upper third of the deltoid muscle in many adults [7].
References
1. Atanasoff S, Ryan T, Lightfoot R, Johann-Liang R. Shoulder injury related to vaccine administration (SIRVA). Vaccine 2010;28:8049-52.
2. Bodor M, Montalvo E. Vaccination-related shoulder dysfunction. Vaccine 2007;25:585-7.
3. Hibbs BF, Ng CS, Museru O, Moro PL, Marquez P, Woo EJ, Cano MV, Shimabukuro TT. Reports of atypical shoulder pain and dysfunction following inactivated influenza vaccine, Vaccine Adverse Event Reporting System (VAERS), 2010-2017. Vaccine. 2019 Nov 26. pii: S0264-410X(19)31546-4. doi: 10.1016/j.vaccine.2019.11.023. [Epub ahead of print] PubMed PMID: 31784231.
4. Sever JL, Brenner AI, Gale AD, Lyle JM, Moulton LH, Ward BJ, West DJ. Safety of anthrax vaccine: an expanded review and evaluation of adverse events reported to the Vaccine Adverse Event Reporting System (VAERS). Pharmacoepidemiol Drug Saf. 2004;13:825–40.
5. Institute of Medicine. In: Stratton K, Ford A, Rusch E, Clayton EW, eds. Adverse Effects of Vaccines: Evidence and Causality. Washington (DC): National Academies Press (US); 2012.
6. Hesse EM, Atanasoff S, Hibbs BF, Adegoke OJ, Ng C, Marquez P, Osborn M, Su JR, Moro PL, Shimabukuro T, Nair N. Shoulder Injury Related to Vaccine Administration (SIRVA): Petitioner claims to the National Vaccine Injury Compensation Program, 2010-2016. Vaccine. 2019 Nov 23. pii: S0264-410X(19)31557-9. doi: 10.1016/j.vaccine.2019.11.032. [Epub ahead of print] PubMed PMID: 31771864.
7. Cook IF. Evidence based route of administration of vaccines. Hum Vaccin 2008; 4:67-73.
8. Cross GB, Moghaddas J, Buttery J, Ayoub S, Korman TM. Don't aim too high: Avoiding shoulder injury related to vaccine administration. Aust Fam Physician. 2016 May;45(5):303-6.
9. Cook IF, Williamson M, Pond D. Definition of needle length required for intramuscular deltoid injection in elderly adults: an ultrasonographic study. Vaccine 2006;24:937-40.
10. Poland GA, Borrud A, Jacobson RM, McDermott K, Wollan PC, Brakke D, Charboneau
JW. Determination of deltoid fat pad thickness. Implications for needle length in adult immunization. JAMA 1997;277:1709-11.
* Reproduced with permission from The Royal Australian College of General Practitioners from: Cross GB, Moghaddas J, Buttery J, Ayoub S, Korman TM. Don’t aim too high: Avoiding shoulder injury related to vaccine administration. Aust Fam Physician 2016;45(5):303-6. Available at www.racgp.org.au/afp/2016/may/don’t-aim-too-high-avoiding-shoulder-injury-related-to-vaccine-administration/